UX RESEARCH
The Invisible Second User - a healthcare portal designed for the family caregiver
5
Research-backed design principles
4
Competitor tools torn down
2
Rounds of usability testing
The problem
Almost every healthcare app is built on one assumption: one account, one patient, and the patient is the person tapping the buttons. That is not how care actually works. A huge amount of it is run by family members. A parent tracking a child's medication. An adult child booking a specialist for an aging parent. A spouse managing someone's recovery.
These people are an invisible second user. The software does not know they exist. So they share logins they are not supposed to, translate medical English for the person they care for, and juggle a stack of separate portals on one phone. When something slips, a missed med, a missed appointment, the system blames the patient. It is not a patient problem. It is a design problem.
I am a caregiver myself, so I have watched this up close. This project asks one question: how should these tools be built when the user is not the patient, but the person looking after them?
Who it's for
Meet Amara, 38. She manages healthcare for her two kids, including Noah, who has ongoing needs. She runs all of it from her phone, in the gaps of a normal day. She is not the patient. Every screen she touches was built as if she were.
Amara is not an edge case. In my research, a family physician estimated at least a third of his consultations involve a relative steering the care, not the patient. Amara is who the framework is built for.

What's already out there
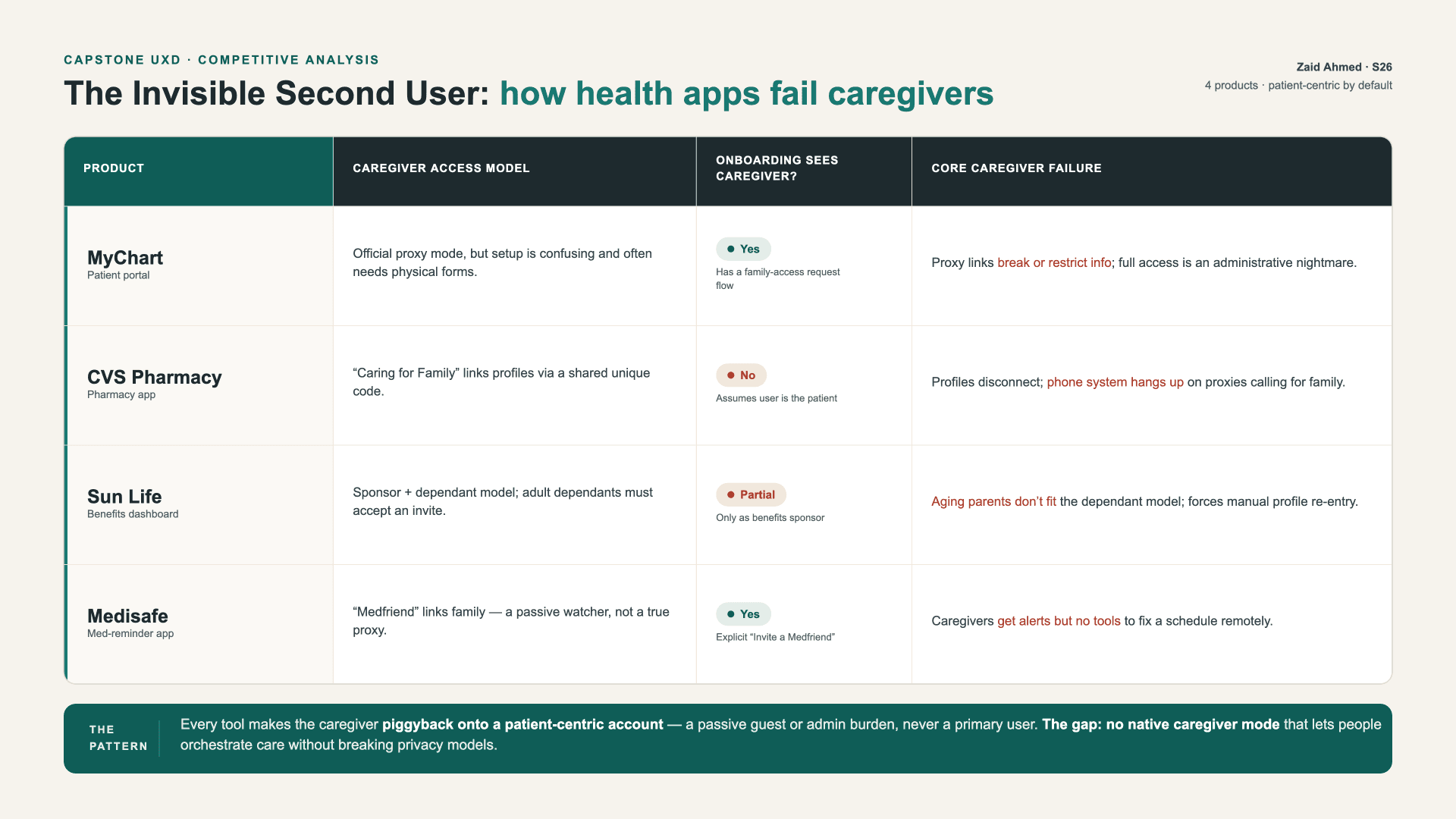
I tore down four tools caregivers actually use, looking specifically at where each one fails the second user.
MyChart (patient portal). Has official proxy access, but setup is confusing, often needs paper forms, and proxy links break or restrict information. For a teen, a parent can be limited to paying bills and booking, with results hidden.
CVS pharmacy app. Has a "Caring for Family" link, but onboarding assumes you are the patient, and the phone system has been known to hang up on caregivers calling for a relative.
Sun Life (benefits dashboard). Built on a sponsor-and-dependant model. Aging parents do not fit it, and you re-enter dependants by hand even when they share your plan.
Medisafe (med reminders). Its "Medfriend" feature only pings the caregiver after something has already gone wrong. It cannot let them step in and fix the schedule.
The pattern under all four: every tool makes the caregiver piggyback onto a patient's account, as a guest or an admin chore, never as a real user with their own identity, tasks, and consent.
That gap is the value proposition. None of these treat the caregiver as a first-class user. My framework gives a product team the principles and patterns to design for that second user without breaking privacy models or leaning on shared passwords.
The research
Alongside the teardown, I ran three interviews, each from a different seat in the problem: a family caregiver managing two kids across three portals, a healthcare professional who sees the gap from inside the system, and a designer who has built patient-facing healthcare tools. The questions were built around past behavior, not opinions, so instead of "would an app like this help," I asked things like "walk me through the last time you booked an appointment for someone you care for."
A few things came back loud and clear:
Logins get shared. The family caregiver keeps every account under his own login and hands one master password to his wife.
Tasks drop in the gaps. They missed a speech therapy appointment because each parent assumed the other had booked it, then paid a cancellation fee and waited two months for another slot.
Clinical language creates panic. The physician described caregivers seeing a raw, slightly abnormal result with no context and spiralling, when all they needed was "the doctor reviewed this, no action needed."
Systems talk to the wrong person. Appointment reminders get addressed to children who do not own phones, so the texts land on the parent the system refuses to acknowledge.
Those four pains map straight onto the five principles below.
Five principles
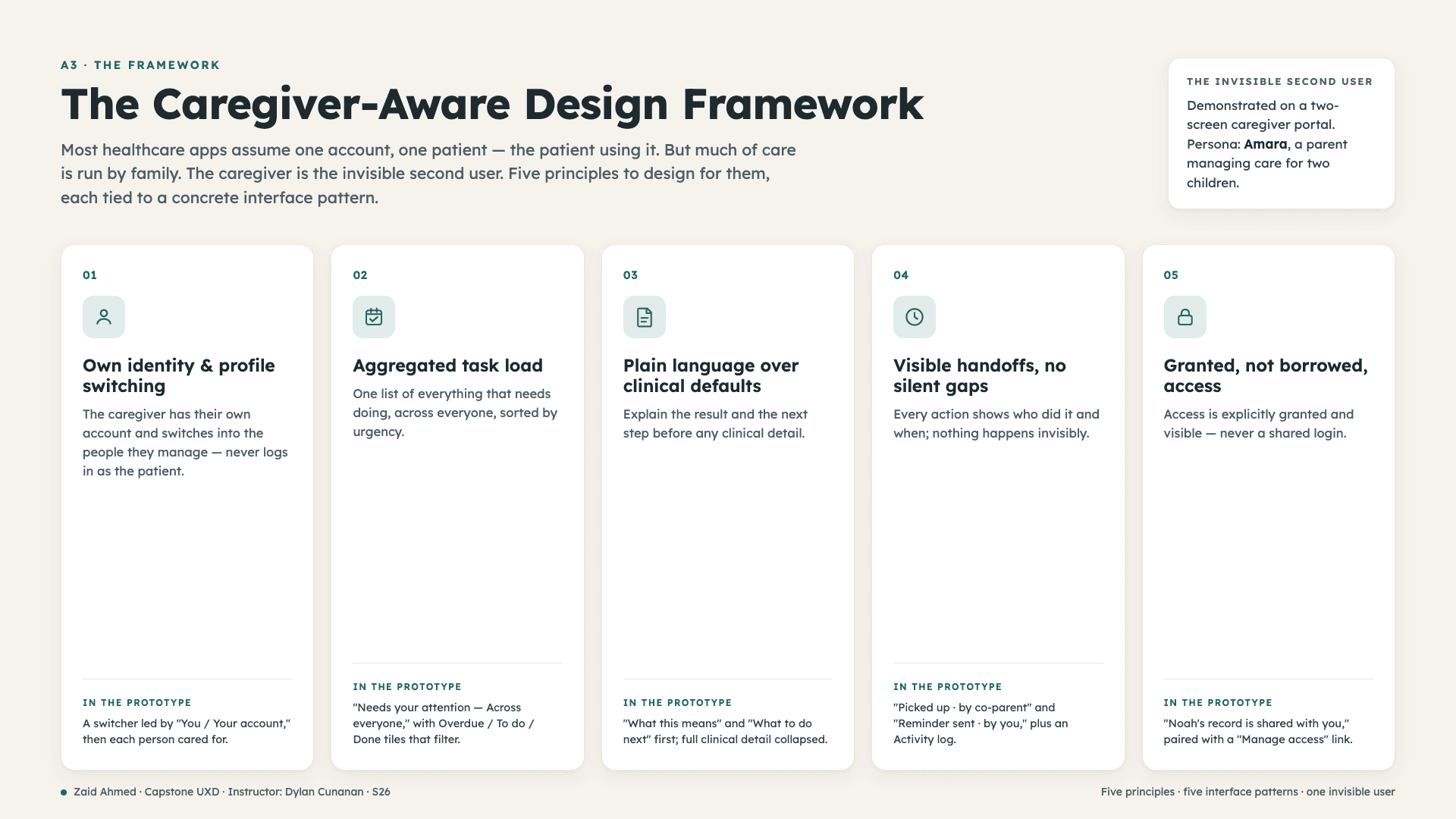
The framework turns that research into five principles, each tied to a concrete interface pattern, demonstrated on a two-screen caregiver portal.
Own identity and profile switching. The caregiver gets their own account and switches into each person they manage, instead of logging in as the patient. Home puts "You / Your account" at the top, separate from the people cared for.
Aggregated task load. One list of everything due, across everyone, sorted by urgency, with Overdue, To do, and Done tiles that filter it.
Plain language over clinical defaults. Lead with what a result means and what to do next. Keep the full clinical detail one tap away instead of forcing it on everyone.
Visible handoffs, no silent gaps. Every action shows who did it and when. "Picked up by co-parent, 11:05 AM," plus a running activity log per item.
Granted, not borrowed, access. Access is explicitly granted and visible, never a shared password. The record tells the caregiver why they can see it and lets them manage who else can.
The first build, and what testing broke
I skipped low-fidelity wireframes and went straight to a working prototype, then treated that first build as the thing to test and tear apart rather than something precious.
Round 1 was an expert heuristic evaluation against Nielsen's heuristics and my own five principles. It produced eight findings and a change list. The sharp ones: the caregiver's own profile was missing from the switcher, status tiles looked tappable but did nothing, handoff attribution contradicted itself, and a muted text color failed WCAG AA contrast. I fixed each in a revised build: added "You / Your account" to the switcher, made the tiles filter, made every handoff show one actor and time, and darkened the muted token to clear roughly 7 to 1 contrast.
What real caregivers did with it
Round 2 was a moderated usability test with three caregivers, one task per principle, think-aloud, on the revised build. All three got through the core tasks with ease scores of 6 and 7 out of 7.
The most useful finding was an uncomfortable one. All three expected the profile switch to be functional: tap a person and the whole view should change, and their own profile should be editable, not a fixed label. One put it plainly: "the switch button was straightforward, but I assumed I'd be able to actually switch the account." That undercuts how Principle 1 currently executes, and I am keeping it visible rather than smoothing it over, because it is the clearest signal of what to build next. Two smaller issues showed up: one participant could not find "Manage access," and one mixed up similar-looking task cards.
What held up: the plain-language result raised zero problems, the switcher itself was easy to find, and reception was strong. Unprompted, a participant said the same pattern would work for banking, insurance, and taxes.
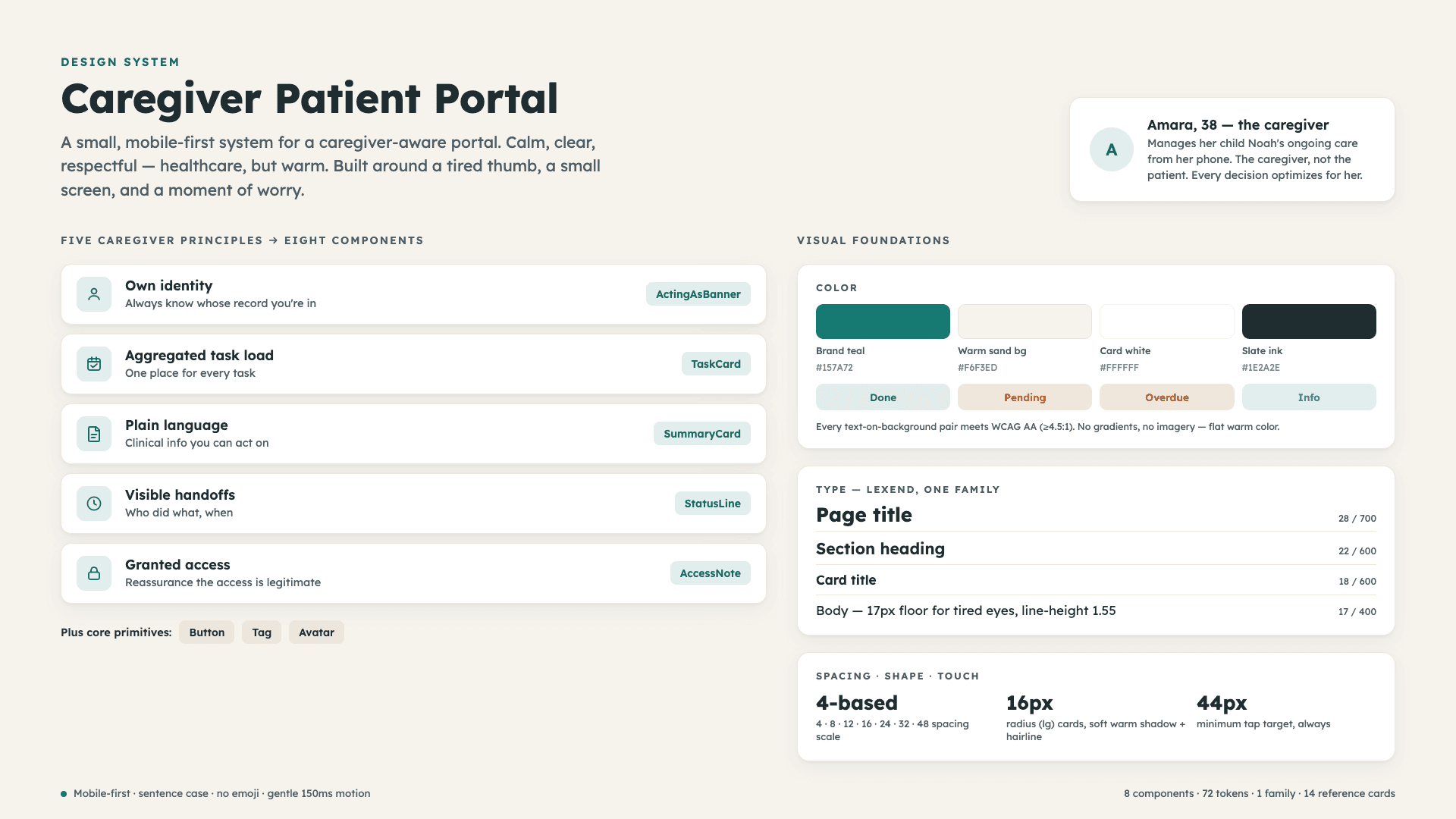
The design system
The portal runs on a small, mobile-first design system built for a tired thumb and a stressed moment: calm, clear, and warm rather than clinical. Five caregiver principles mapped to eight components, one type family, a warm off-white base, and a color set where every text-on-background pair clears WCAG AA. No gradients, no stock imagery, flat warm color.
What's next
Round 2 wrote my next change list. Make selecting a person actually switch context, or state plainly why the home view stays "across everyone," and make the caregiver profile editable. Raise the visibility of "Manage access" on the record. Differentiate the task cards by type, with distinct labels and icons for a refill, an appointment, and a reminder. Past that, the honest gaps: empty and error states, and a larger testing round, because three participants is directional, not proof.
Why this matters
Patient-centered design is the default in healthcare UX. Almost no one designs for the caregiver, even though a large share of the people using these tools are doing exactly that. This project names that second user and hands a product team five principles, four competitor teardowns, and two rounds of testing they can pick up and use.
And it may not stop at healthcare. The strongest moment in testing was a caregiver realizing, on her own, that managing someone else's banking, insurance, and taxes has the same shape: your own identity, switching into someone you are responsible for, granted access, and a clear record of who did what. The invisible second user is everywhere. Healthcare is just where it hurts most.
portfolio
Other projects
Check out some of my other work


